




WElcome TO
Explore our blog that focuses on holistic care for any and all ages - pediatric well-being, pre/post-natal health, and adult vitality.
THE BLOG


Are you feeling frustrated or even disheartened because your child seemed to be making incredible progress with their neurological challenges, and then suddenly… everything stalled? Maybe you’ve even noticed some regression even. Behaviors returning that you thought were gone forever, sleep disruptions creeping back in, or emotional regulation challenges resurfacing.
If you’re wondering if the care plan is failing or if something’s wrong, we want you to take a deep breath and hear this: plateaus and even regressions are often a normal and necessary part of the healing process.
The neurological healing journey is rarely a straight line. In fact, it’s more like a rollercoaster with its fair share of ups, downs, and unexpected twists. But here’s the thing parents often miss – those plateaus aren’t signs of failure. They’re actually evidence that your child’s nervous system is working through deeper layers of dysfunction and adapting to a new level of organization.
You’re Not Alone in This Journey
As neurologically-focused chiropractors, we see this pattern daily in our practice. Nearly every parent who brings their child for care will experience what research refers to as “non-linear healing progress.” Research on neuroplasticity shows that the brain has the ability to reorganize itself, forming new connections and, in some instances, even generating new neurons.
Children typically experience periods of rapid advancement followed by consolidation phases where skills are integrated. The same pattern applies to neurological healing, where the “two steps forward, one step back” progression isn’t a failure. It’s actually the brain’s natural way of reorganizing and creating lasting change.
Understanding the Five Main Causes of Healing Plateaus
Let’s walk you through the most common reasons why your child might be experiencing a plateau, so you can understand what’s happening and feel confident moving forward.
1. Growth Spurts and Developmental Milestones
When your child is growing rapidly or mastering new developmental skills, their body’s energy and resources may be directed toward physical growth and neural integration. During growth spurts, your child’s body is working intensely to lay down new bone, muscle, and neural tissue. Requiring tremendous energy that may temporarily be diverted from other healing processes.
This can show up as:
- Increased moodiness
- Disrupted sleep patterns
- Temporary regression in other areas as their nervous system focuses on integrating these physical changes
Remember that these growth-related pauses are ultimately signs of progress, not setbacks. Each time your child’s nervous system successfully integrates a new skill, it becomes more resilient overall.
2. Immune Challenges and Their Healing Effects
Here’s something that might surprise you: fevers and illnesses aren’t simply obstacles to progress – they’re sophisticated neurological responses that can actually accelerate healing in the long run.
When a child has a fever, their immune system triggers the hypothalamus’s thermoregulatory center, leading to an increase in body temperature. This activates immune cells and creates an environment that’s inhospitable to pathogens. During this process, the nervous system diverts resources to orchestrate the immune response, which can temporarily manifest as lethargy, irritability, or a seeming disconnection.
But here’s the fascinating part: the fever process stimulates the release of neurotrophic factors. Special proteins that support neuronal growth and plasticity – potentially accelerating neurological development after recovery. This is why we often see major breakthroughs following an illness, though there may be a brief regression immediately after.
3. Environmental Factors: The Hidden Disruptors
Children with pre-existing neurological challenges often have nervous systems that are already dysregulated, making them more sensitive to environmental toxins. From pesticides and heavy metals in food to flame retardants in furniture and VOCs in cleaning products, these accumulated toxins can disrupt normal neurological function.
Mold exposure, whether from hidden leaks or poor ventilation, releases mycotoxins that can lead to cognitive impairments and neurological symptoms. These environmental stressors can contribute to temporary plateaus in progress as the body works to process and eliminate these substances.
4. Emotional Stress and Life Changes
Major transitions like starting a new school year or subtle shifts in family dynamics can trigger the sympathetic “fight or flight” response in children with neurological challenges. This stress response releases hormones like cortisol and adrenaline, which can quickly become overwhelming for children with pre-existing nervous system dysregulation.
Over time, this chronic state of stress can contribute to developing subluxation – areas of dysfunction within the nervous system that further perpetuate the cycle of dysregulation. This is why we often see regressions during periods of change or high emotion. The nervous system is allocating resources to manage the perceived stress rather than continuing to make developmental progress.
5. Medication and Therapy Overload
Many medications are designed to suppress or override the symptoms rather than resolve the root cause of neurological dysfunction. They act like a “mute button” for symptoms the body is still struggling with underneath. When we begin true healing by restoring brain-body communication and balancing the nervous system, it’s like the body begins to “wake up” again, sometimes temporarily resurfacing underlying patterns.
The nervous system has a limited capacity, which is why we recommend prioritizing nervous system regulation first and then gradually layering in additional therapies.
What This Means for Your Family
At RCW, we understand that, most of the time, plateaus are simply one or more of these outside stressors putting a bit of a headwind in play. Once that stressor passes and your child builds up additional resilience and adaptability, they’ll blow right past it and be right back on the path to progress and breakthrough once again.
The key is understanding that healing is non-linear. It’s a lot of “two steps forward, one step back” at first! Growth spurts, immune stress, environmental toxins, emotional changes… all of these can cause temporary plateaus or even regression as your child’s nervous system works hard behind the scenes to integrate and level up.
Moving Forward with Confidence
That 3-week sleep regression, the return of meltdowns, the clinginess that came out of nowhere – it’s not a sign that care isn’t working. It’s actually one of the clearest signs that your child’s nervous system is unwinding and releasing! Just like cleaning out your closet or pantry, it gets a little messier before we can reorganize it all into pretty containers.
You’re doing better than you think, and their nervous system is too. Trust the process, stay consistent with your care plan, and remember that these apparent setbacks are often evidence of your child’s nervous system working through deeper layers and preparing for the next breakthrough.
If you are ready to take the next step in your child’s neurological healing journey, or if you’re experiencing these plateaus and want some guidance, please reach out to RCW today!


There are so many emotions to navigate through when finding out you’re pregnant. Whether you have longed for a positive pregnancy test or this was a complete surprise, emotions and thoughts flow through your brain at what seems to be 1000 mph. “Is it a boy or girl?! How will my body do this? Who do I need to call and tell first?! How will we announce it on Instagram? What about the nursery? Will they go to private or public school? When do we start a college fund….???” It’s like everything starts to spin out of control and escalate. The list really does seem never-ending! And don’t get us started on the number of opinions and questions that start to flood in after telling people the good news!
Take a deep breath. Everything is going to be okay.
Let’s start with two of the most important questions to ask yourself first:
- “What kind of pregnancy do I want?”
- “Who is going to help me achieve that?”
In this article, we will explore what prenatal chiropractic is, the common (BUT NOT NORMAL) symptoms of pregnancy, and the available care options to create the healthiest human beings.
What is Prenatal Chiropractic?
Prenatal chiropractic care is a specialized form of chiropractic that encompasses two (2) different elements that greatly benefit both mom and baby on this incredible journey:
- We provide safe, gentle, and effective adjustments that help mom’s nervous system better relax and make room for the growing baby, and keep mom strong and ready for a natural birth and optimal transition to motherhood
- Our office also provides an incredibly empowering and supportive environment where expecting moms and dads can ask the tough questions, access incredible resources, and feel confident throughout their journey
Taking it one step further, the kind of chiropractic care we provide goes beyond just typical structural-based chiropractic care and focuses entirely on mom’s nervous system.
The umbilical cord connecting that developing baby to mom is not just there to carry oxygen and nutrients, but it’s also the neurological “power cord” that connects mom’s nervous system to her baby’s. In today’s world, where we have more stress, tension, and anxiety than ever before, the neurologically-focused prenatal chiropractic care that we offer, therefore acts as a crucial component of keeping both mom and baby’s nervous system healthy, calm, and clear of interference all along the way!
What are the Common Health Challenges Faced During Pregnancy?
During pregnancy, a woman’s body undergoes significant changes, neurologically, hormonally, and physically, to accommodate the growing baby. These changes can lead to various hormonal changes, nervous system imbalances, and neuromuscular issues. There are many symptoms that commonly come along with pregnancy. From the early stages of morning sickness and fatigue to the annoying struggles of reflux, heartburn, trouble breathing, and the body changes, such as lower back pain, pelvic discomfort, and postural imbalances. All of these are very common during pregnancy, but are they normal?
What Causes All of These Pregnancy-Related Health Challenges?
This may seem like a silly question. The obvious answer is that you are growing a brand new beautiful baby from scratch. A little more… Every. Single. Day. OF COURSE YOU’RE FATIGUED AND UNCOMFORTABLE! But let’s dive deeper into the root causes of what is really causing some of these symptoms and what we can do about it!
The Role of the Nervous System in Pregnancy
A regulated and well-balanced nervous system is of utmost importance during pregnancy. It profoundly influences both the expectant mother’s health and the developing baby’s well-being. The nervous system acts as the master control center. Coordinating and regulating all body functions, from basic physiological processes to complex hormonal interactions. And now your nervous system has to do “double” the job, controlling all of your bodily functions and baby’s too.
During pregnancy, the autonomic nervous system (ANS), which is responsible for involuntary actions, plays a crucial role. The ANS consists of two branches: the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS). The SNS is what comes to life when you are under duress and experiencing stress. You might have heard it referred to as fight or flight. The PNS is the branch that helps us calm down, relax, and function once again after the stress has passed. To learn more about the parasympathetic nervous system and the vagus nerve that controls and regulates most of it, check out this additional article here.
But this wildly important parasympathetic side of the nervous system is not just responsible for rest and relaxation; it’s in charge of growth and development as well. Making it perhaps the single most important system to pay attention to during the prenatal period (and postpartum as well). If mom’s nervous system is not in optimal growth and development mode, how can baby’s be?
A well-regulated and optimally balanced nervous system is essential for both mom and baby’s optimal well-being. When the nervous system is in a state of balance, it promotes better hormonal regulation, blood flow, and immune function, creating an optimal environment for the baby’s growth and development. It also contributes to the mother’s overall well-being, reducing stress levels, promoting relaxation, and improving sleep quality.
The Role of Stress and Subluxation in Pregnancy
Unfortunately, an imbalanced or dysregulated nervous system can lead to various health challenges during pregnancy. High levels of stress and anxiety lead to constant activation of the SNS and can contribute to complications like elevated blood pressure, decreased blood flow to the placenta, and potential adverse effects on fetal development.
Experiencing occasional stress is as normal as it gets, but unfortunately, today, too many women experience moderate to high levels of stress far too often. And sadly, our current medicalized system of prenatal care only adds to that stress, fear, anxiety, and disempowerment, it seems, with each and every visit to the doctor, additional ultrasound or exam, and so forth.
This ongoing and overwhelming stress is called subluxation. When subluxation is present, the entire nervous system shifts into an excessive sympathetic dominant state. Increasing the tension on not just the nerves and muscles but also organs, glands, digestive system, and more. It even leads to its own “perfect storm” vicious cycle where now stress and anxiety are increased once again, other health challenges and concerns set in, and more trouble brews as the pregnancy goes on.
This tension can exacerbate blood pressure issues, back pain and sciatica, neck pain and headaches, anxiety and nausea, hormonal imbalances, and even affect a baby’s position in the womb.
Drug-Free Care Options for Pregnancy-Related Health Challenges
Fortunately, there are care options available to help pregnant women manage their stress and greatly improve their quality of life while their bodies are adapting to these new changes.
Often by the time pregnant women learn about the things we just covered with subluxation and the nervous system, they have tried all of the medications, homeopathics, teas, nutrition hacks, and physical therapies for pregnancy symptoms like heartburn, reflux, morning sickness, and pelvic pain.
As most of these things are great, they aren’t fully addressing the root causes of pregnancy-related health challenges. If you want to tackle these issues head-on and not only reduce the symptoms and health challenges you’re experiencing but also optimize your entire body and nervous system throughout the pregnancy, then neurologically-focused prenatal chiropractic is perfect for you!
Can You Measure This Stress and Subluxation? Introducing HRV to Prenatal Care
It’s quite an exciting time to be at the forefront of prenatal care like we are! In the past few years, we’ve not only seen more and more research prove how important neurological health is during the prenatal journey (for both mom and baby), but also, some incredible technology has been developed to help us track and measure your neurological health all along the way in just a matter of minutes!
This technology is called HRV, which stands for Heart Rate Variability. It is an absolutely essential exam for all pregnant women to take on a regular basis because it provides valuable insights into the health and function of their autonomic nervous system (ANS) function and overall health during pregnancy.
As stated above, the ANS controls and regulates every vital function in the body. Including heart rate, respiratory rate, digestion, and more. With “fight or flight” and “rest and relax” being the two main branches of the ANS, it’s important to track how it is functioning and whether things are out of balance or not.
HRV is a measure of the variation in time between consecutive heartbeats. A higher HRV indicates a more flexible and adaptable nervous system, which is associated with better overall health and resilience to stress during pregnancy. This also means reduced maternal stress, better sleep quality, improved cardiovascular health, and enhanced immune function. Additionally, maintaining a balanced ANS is essential for supporting proper blood flow to the placenta and optimal fetal development.
On the other hand, a lower HRV suggests an imbalanced or stressed ANS, which can lead to various health issues, commonly leading to a high-risk pregnancy.
Therefore any professionals working with pregnant women need to be using HRV technology as the foundation of their care protocols and programs. Allowing them to not only establish a baseline at the onset of care but also to track and monitor progress via actual neurological change and improvement.
Measuring and tracking true autonomic nervous system and vagus nerve functions are, therefore, the foundation of our work as Prenatal PX Doctors. Each and every pregnant woman who walks into our offices first get an HRV test to measure their overall adaptability and parasympathetic or vagal nerve tone.
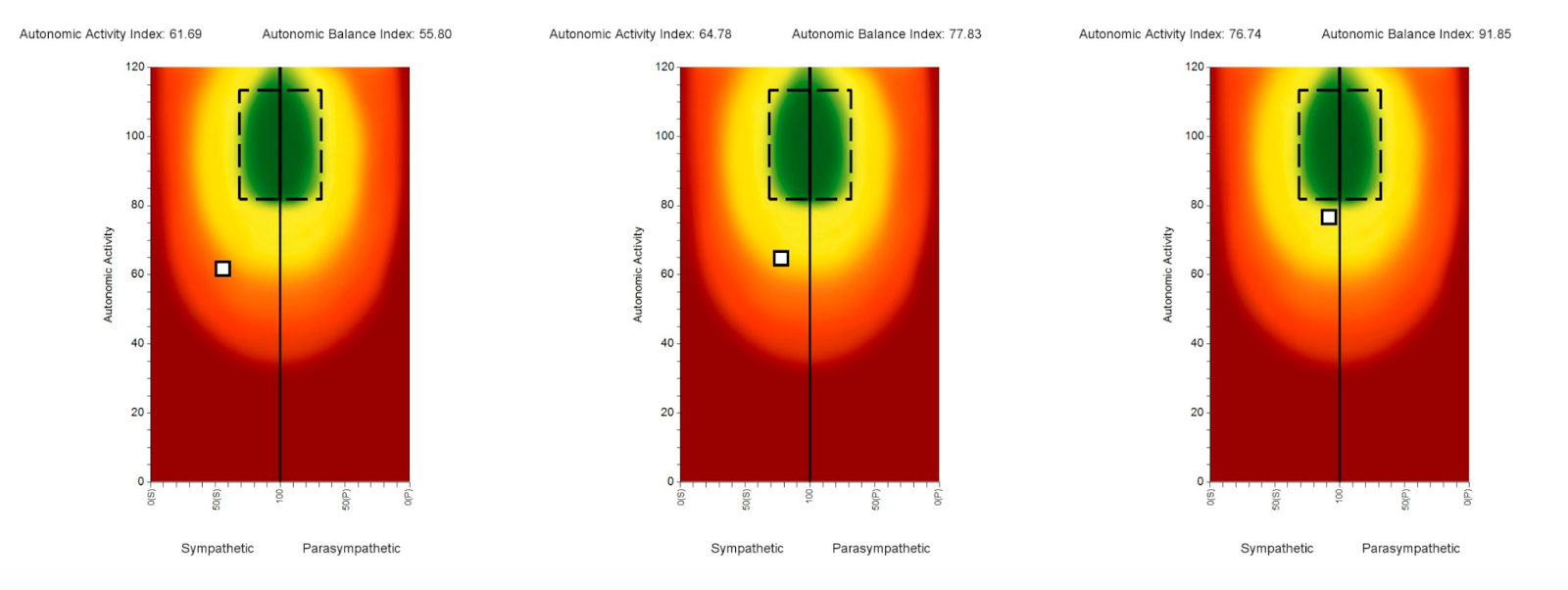
Below is an image with a series of three (3) HRV Scans performed on a pregnant woman throughout her pregnancy. The first scan on the far left shows the small white box way in the lower left quadrant of the HRV plot, indicating her parasympathetic nervous system and vagus nerve are both suppressed and shut down, allowing her sympathetic fight or flight system to run out of control.
Then as care progresses over the second and third trimester, you can see the white box move towards the center line and higher up towards the green circle, indicating that her subluxation and dysautonomia were vastly improved and her nervous system is now much calmer, balanced, and better regulated, which shows that she is more adaptable to the stressors of pregnancy and ready to conquer her birth!
More Stress to Measure
In addition to HRV, we ALSO run two (2) additional tests. NeuroThermal and NeuroSensory EMG, to complete the overall INSiGHT Scans and neurological exam. Together these three (3) collective scans can function as a pregnancy test that actually looks beyond symptoms, and dives deep into the nervous system and how prenatal chiropractic can help both mom and baby.
Once we have these incredible INSiGHT Scans done, we can then put together a fully customized and personalized care plan made uniquely for the pregnant woman’s corresponding trimester. Once care begins, each and every neuro-tonal adjustment our doctors are trained to make is designed to address subluxation and dysautonomia directly.
By activating and stimulating the vagus nerve and parasympathetic nervous system repeatedly over a period of many weeks to months, we then start to see an incredible decrease in the sustained sympathetic storm so many pregnant women are stuck in.
The first improvements these women typically notice are with sleep, digestion, fewer aches and pains, less “pregnancy brain,” more energy, and more focus. From there, the brain and nervous system can get back on track developmentally, and benefit both mom and baby, leading to optimal development and baby positioning, which can result in a quicker birth, fewer interventions, more vaginal births, and can help seek to prevent The Perfect Storm.
HOW TO GET THE HELP YOU NEED
Being pregnant can be one of the most rewarding, exciting, and joyous times of our lives. But it can also feel very scary and overwhelming. Just remember that you are not alone, and you have choices when it comes to the pregnancy that you want and to the type of healthcare that you want supporting you along the way.
The earlier you are able to optimize and improve your neurological function, the better your pregnancy and birth outcomes will be for both you and your baby.
The best place to start on this journey is with a consultation and HRV test. Get scheduled for an empowering consultation, INSiGHT Scans, and HRV right away!
Remember, you are not alone in this pregnancy journey, and we’re on your team! Take the first step and find the doctor, the care, and the community you and your baby deserve.



Have you ever noticed how your baby seems perfectly content in your arms, but the moment someone else holds them, the waterworks begin? Or how does your little one somehow sense when you’re stressed and respond in kind? Or why healthcare providers prioritize skin-to-skin contact right after birth?
It’s not a coincidence—it’s co-regulation. And it might just be the most powerful tool in your parenting toolkit.
We want to share with you the absolute best hack when it comes to soothing a colicky baby, bringing down a fever naturally, and even boosting your milk supply. Would you believe it’s all the same approach?
What Is Co-Regulation (And Why It’s Your Parenting Superpower)
Let us let you in on a little secret: your nervous system controls everything, and your baby’s nervous system is deliberately underdeveloped at birth. This isn’t a design flaw—it’s by design! Babies need their parents to help regulate, calm, and nurture them.
Your calm presence isn’t just emotionally comforting—it actually provides the neurological pattern your baby’s developing brain needs to learn regulation. When you hold your baby close, their heart rate, breathing patterns, and stress hormone levels literally synchronize with yours. It’s a beautiful biological dance that sets the foundation for lifelong health and emotional well-being.
The first three years of life represent a critical period for brain development, with more than 1 million new neural connections formed every second. Studies clearly show that babies receiving regular skin-to-skin contact have better temperature regulation, improved breastfeeding success, and significantly less crying.
This is all called co-regulation, and it truly is the best “hack” when it comes to anything baby-related!
Understanding the Nervous System Connection
Think of your nervous system like a car:
- Your sympathetic system is the gas pedal—revving up your heart rate and stress hormones when you perceive danger or stress.
- Your parasympathetic system (primarily activated by the vagus nerve) is the brake pedal—slowing things down and promoting relaxation.
Your baby is remarkably aware of your nervous system state. They’re not reading your words or even your intentions—they’re picking up on subtle cues through your facial expressions, voice tone, heart rate, breathing pattern, and the quality of your touch.
When you’re stressed, your baby often becomes stressed too. When you’re calm, your baby can borrow your calmness until they develop their own regulation skills.
Why Co-Regulation Doesn’t Always Come Naturally
Sometimes, despite our best efforts, co-regulation doesn’t seem to work. Your baby remains fussy despite your cuddles, or you find yourself struggling to maintain the calm your baby needs.
This isn’t your fault! Several factors can create a “perfect storm” that affects co-regulation:
- Fertility struggles and the stress they bring
- High maternal stress during pregnancy (which floods the developing baby with stress hormones through the umbilical cord)
- Birth interventions like C-sections, forceps, and vacuum extraction that can create physical tension in the delicate neurospinal structures of both mother and baby
This physical tension can cause subluxation—areas of neurological dysfunction that interfere with proper nerve communication. Particularly affecting the vagus nerve and autonomic balance.
Without addressing these root neurological issues, babies don’t simply “grow out” of regulation challenges. They often “grow into” other health challenges like sensory issues, digestive problems, and emotional regulation difficulties.
How Neurologically-Focused Care Can Help
When co-regulation isn’t happening naturally, Neurologically-Focused Chiropractic Care can help restore balance to both your nervous systems:
- Comprehensive neurological scans (INSiGHT Scans) can objectively measure nervous system function in both mother and baby
- Gentle adjustments address areas of subluxation and restore proper neurological function
- As neurological function improves and vagus nerve function is restored, dramatic improvements often follow in sleep patterns, feeding behaviors, emotional regulation, and overall contentment
The Journey Forward
The journey of motherhood is absolutely amazing and such a blessing… but that doesn’t mean it isn’t hard sometimes! You’re not meant to do this alone, and seeking support isn’t a sign of weakness—it’s a sign of wisdom.
Co-regulation isn’t just a parenting technique; it’s a biological necessity for your baby’s developing nervous system. By understanding and nurturing this connection, you’re giving your child the neurological foundation for lifelong health and emotional well-being.
At RCW, we understand that your ability to co-regulate improves when your whole family’s nervous systems are functioning optimally. When everyone is regulated, the ripple effect creates a harmonious environment where your baby can thrive.
If you’re ready to take the first step and schedule a consultation, please don’t wait and reach out to us today!
You already have everything you need to be the calming force in your baby’s life. Trust your instincts, honor the power of your connection, and remember that in those moments when your baby finds peace in your arms, you’re not just soothing them—you’re literally shaping their developing brain in the most beautiful way possible.
Now that’s a superpower worth celebrating!

Dad, Are You Running on Empty?
I want you to take a moment right now and ask yourself: When was the last time you felt truly energized? Not coffee-jittery or adrenaline-pumped, but genuinely rested and ready to tackle both work and family life?
If you’re drawing a blank, you’re not alone. Nearly 15% of fathers are experiencing perinatal (before, during, and after pregnancy) anxiety, and up to 50% of dads face postpartum depression alongside their partner. That “dad bod” everyone jokes about? It’s not just about skipping the gym—it’s your body trying to tell you something critical about your nervous system.
The Truth About Dad Stress (That Nobody’s Talking About)
Here’s what’s happening: Your nervous system has two primary modes—the sympathetic “fight or flight” response and the parasympathetic “rest and digest” state. When you’re constantly juggling work deadlines, family responsibilities, financial pressures, and trying to maintain relationships, your body gets stuck in sympathetic dominance. You’re essentially driving with the gas pedal pressed to the floor 24/7.
This chronic activation causes your body to continuously release cortisol and other stress hormones. While these hormones are life-saving in true emergencies, they create serious health problems when constantly elevated. Your nervous system wasn’t designed to handle this level of sustained stress, leading to what we call dysautonomia—a dysfunction in the autonomic nervous system that impacts nearly every bodily function.
The Cascade Effect: How Stress Impacts Everything
Chronic sympathetic dominance and elevated cortisol directly contribute to:
- Increased abdominal fat and muscle loss (the infamous “dad bod”)
- Suppressed testosterone production
- Reduced muscle recovery
- Disturbed metabolic function
- Inflammation affecting everything from cardiovascular health to immune system
- Brain fog, memory issues, reduced patience
- Diminished ability to regulate emotions
These aren’t character flaws—they’re neurological responses to chronic stress.
Why Traditional Self-Care Advice Often Falls Flat
Here’s where many well-meaning health advice givers miss the mark. They tell you to “just exercise more” or “eat better,” but when your nervous system is already exhausted, finding the energy to implement these changes feels impossible.
The cruel irony? You need these healthy behaviors to heal, but chronic stress has depleted the very reserves you need to start these practices. This is why willpower alone isn’t enough—you need to address the root cause of your fatigue at the neurological level first.
Until your nervous system shifts out of survival mode, sustainable lifestyle changes remain extremely difficult to implement and maintain.
The Dad Health “Cheat Code”: Neurologically-Focused Chiropractic Care
Here’s where the game-changer comes in. Neurologically-focused chiropractic adjustments directly address subluxation—neurological interference that keeps your nervous system stuck in stress mode.
These gentle, precise adjustments help restore proper communication between your brain and body, allowing your nervous system to finally shift out of fight-or-flight and into rest-and-recover mode.
This is why dads who receive Neurologically-Focused Chiropractic Care report:
- Better sleep quality
- Improved energy levels
- Reduced pain and tension
- Enhanced mood
- Gradually improving physical health
Think of it as hitting the reset button on your overstressed nervous system—creating the foundation for all other health improvements to build upon.
What Makes This Approach Different
At Rochester Chiropractic and Wellness, we use advanced INSiGHT Scan technology to precisely measure nervous system function and identify exactly where stress and subluxation are impacting you most. This scientific approach allows for personalized care plans based on objective measurements, not just generic recommendations.
The focus is specifically on the neurological component of health rather than just musculoskeletal pain, addressing the root cause of your signs rather than just temporarily masking them.
Dad, You Deserve to Feel Your Best
You deserve to feel your best, not just for your family, but for yourself. Neurologically-focused chiropractic care isn’t just another thing to add to your already overwhelming to-do list. It’s the essential first step that makes everything else possible.
By addressing the root cause of your exhaustion at the nervous system level, you’ll finally have the energy to implement those other healthy habits you know you should be doing.
Countless dads have experienced this transformation. Within just weeks of beginning care, they report better sleep, improved mood, reduced pain, and the return of energy they haven’t felt in years.
Your family needs you at your best, and that starts with taking care of your nervous system health. If you are ready to take the first step, scheduling a comprehensive Neurological INSiGHT Scan, give RCW a call today!
It’s time to stop running on empty. Your best dad years are still ahead of you!



Let us guess… your child doesn’t just have one speed.
One moment, they’re bouncing off the walls — shouting, spinning, climbing on furniture, and melting down when something doesn’t go their way.
The next moment? They’re completely zoned out and disconnected. Blank stare. Can’t follow instructions. It’s like they’re in the room… but not really there.
You’ve tried the parenting books, the behavior and reward charts, maybe even medications — and still, you’re left asking – Why is my child like this?
And more importantly… How do I actually help them?
Looking Beyond the Labels to Find Real Answers
Here’s the truth that most traditional approaches miss: what we label as ADHD or ADD is often just the tip of the iceberg. Underneath those labels are two very different nervous system patterns – what we call “stuck on the gas pedal” and “stuck on the brake pedal.”
Understanding these patterns helps us make sense of not just the symptoms and everyday challenges, but most importantly, the nervous system dysregulation that’s actually causing them.
Two Sides of the Same Coin
The “Gas Pedal” ADHD Type
This child is stuck in “on” mode – flooded with energy, impulsivity, and big emotions that can’t be controlled. They’re constantly moving, talking, fidgeting, and struggling to slow down. Traditional approaches often focus solely on “managing” these behaviors rather than understanding why they’re happening.
The “Brake Pedal” ADD Type
This child is often shut down, exhausted, foggy, slow to process, and overwhelmed by everything around them. They may appear “lazy” or unmotivated when in reality, their nervous system is struggling to engage properly. This type was formerly known as ADD but is now classified as predominantly inattentive ADHD in modern diagnostic terms.
What’s fascinating – and what many parents don’t realize – is how often these patterns evolve into each other over time. The hyperactive child can develop attention issues as they become frustrated with academic challenges, while the inattentive child can become hyperactive from the built-up stress and anxiety of constantly struggling.
The Concerning Reality of Current Approaches
According to the CDC, an estimated 7 million children in the United States have been diagnosed with ADHD. Approximately 3.5 million of these children (about 69%) are currently prescribed medication for the condition.
While medications work for some children, they often come with concerning side effects:
- Sleep problems and insomnia
- Appetite suppression
- Emotional dysregulation and irritability
- Anxiety and nervousness
- Tics or involuntary movements
- Persistent headaches
- Stomach pain and nausea
- Increased blood pressure and heart rate
- Social withdrawal or “zombie-like” behavior
Most importantly, these medications do not address the root cause — which is often a stressed, dysregulated nervous system. This can lead to a cycle of chasing symptoms, adjusting dosages, or adding more medications to address side effects.
Understanding the True Neurological Roots
At the core of both ADHD presentations lies a complex interplay of neurological factors that impact a child’s ability to regulate attention, behavior, and emotions.
The three key elements we find most often are:
- Subluxation & Sympathetic Dominance: Misalignments, tension, and restricted mobility within the neurospinal system that interfere with how the brain and body communicate. These physical disruptions, often stemming from birth trauma or early injuries, create “noise” in the nervous system.
- Nervous System Dysregulation & Dysautonomia: When subluxation persists, it throws the autonomic nervous system out of balance, often leaving children stuck in a heightened “fight or flight” response that makes calm focus nearly impossible.
- Vagus Nerve Dysfunction: The vagus nerve is essential for activating the “rest and regulate” parasympathetic response. When it’s not functioning properly, children struggle to regulate emotions, attention, and behavior.
Hope, Healing, and Transformation Are Possible
Your child isn’t broken. They don’t need more labels. They need answers. They need understanding. And they need a care plan that finally gets it right.
The best part? We can actually measure what’s happening in your child’s nervous system using specialized scans. These Neurological INSiGHT Scans don’t just label — they measure and map out what’s causing the chaos, so a customized, drug-free care plan can be created to help your child calm their brain, regain focus, and thrive.
From Struggle to Superpower
Here’s what every parent needs to know:
Millions of kids today are either struggling with undiagnosed ADHD — or have a diagnosis but are still stuck in the same cycle of symptoms, side effects, and little to no progress.
That’s because most ADHD tests and treatment plans stop at surface-level symptoms. They label the child… but don’t look deeper into the real root cause.
True ADHD struggles begin in the brain and nervous system. And unless we measure what’s happening under the surface, we miss the most important part.
When your child is locked in stress mode neurologically, no amount of behavior charts, medications, or consequences can bring lasting change. But when we help restore balance to the nervous system? Focus can improve. Meltdowns can decrease. Sleep stabilizes. And what was once seen as a disorder can become a superpower.
Taking the Next Step
If you’re tired of guessing… tired of medications that don’t work… or tired of watching your child struggle without answers — it’s time to look deeper. It’s time to turn your child’s struggle into their greatest strength.
At RCW, we take the time to find the root cause that can help your child heal safely and naturally.
Remember: Understanding which kind of pedal your child’s brain is stuck on is the first step in finding the right solution. With the right approach, your child’s unique brain can become their greatest asset rather than their biggest challenge.

Do you find yourself reaching for that third cup of coffee just to make it through the afternoon? Does your child seem constantly wired yet somehow exhausted, struggling to focus at school but unable to wind down at night? You’re not alone—and there’s a reason for it.
What you and your family are experiencing could be a cortisol addiction. This neurological pattern has become increasingly common in our fast-paced world, affecting not just adults but our children too. The good news? Once you understand what’s happening, you can take effective steps to break the cycle and help your entire family thrive naturally.
Understanding Cortisol Addiction: Why Your Family Feels Wired and Tired
Your body has an amazing system designed to help you respond to the world around you. It’s called the autonomic nervous system, and it has two main branches:
- The Sympathetic Nervous System (fight-or-flight): Activates during emergencies, releasing stress hormones like cortisol and adrenaline that increase heart rate, sharpen focus, and prepare you to respond to danger.
- The Parasympathetic Nervous System (rest-digest-restore): Takes over during calm periods, allowing your body to heal, digest food properly, and restore energy.
These systems should work in harmony, with the sympathetic activated only when truly needed and the parasympathetic dominant most of the time. But in today’s world, many families exist in a state of constant sympathetic activation.
Over time, your body can become dependent on these stress hormones just to function—creating a genuine physiological addiction to cortisol. You feel simultaneously wired and exhausted. Your child appears hyperactive yet struggles to focus when needed.
How It All Begins: The Perfect Storm
For many children, this pattern begins earlier than you might think. Birth interventions like forceps, vacuum extraction, C-sections, and even induction can create physical trauma to a baby’s delicate upper neck and brainstem area. This trauma causes subluxation (misalignment, tension, and neurological interference in the nervous system) and impacts the vagus nerve—the master regulator of the parasympathetic system—and shifts a child into sympathetic dominance right from the start.
This neurological imbalance often manifests first as colic, reflux, or sleep issues in infants. As children grow, it can evolve into focus issues, hyperactivity, emotional dysregulation, and behaviors commonly diagnosed as ADHD or anxiety.
Modern life makes everything more challenging:
- Screens emit blue light that triggers cortisol production and disrupts sleep cycles
- Processed foods spike and crash blood sugar, creating stress on the body
- Packed schedules leave little downtime for parasympathetic recovery
- Constant digital stimulation keeps the nervous system activated
Children with already dysregulated nervous systems often seek intense stimulation (risk-taking behavior, screen time, sugar) to get the dopamine and cortisol their brains are craving. Parents mirror this pattern with caffeine dependence, busy schedules, and their own screen habits.
Together, these factors create family-wide patterns of sympathetic dominance that become increasingly difficult to break.
The Medication Trap: Why Conventional Approaches May Not Be Working
When children display signs of sympathetic dominance like hyperactivity, difficulty focusing, or emotional outbursts, they’re often prescribed stimulant medications such as Adderall or Ritalin. These medications temporarily boost focus by further activating the sympathetic nervous system.
While these medications might provide short-term symptom relief, they don’t address the underlying neurological imbalance. In fact, they can reinforce the body’s dependence on sympathetic activation, potentially making the long-term situation more challenging.
As parents, we often don’t realize we’re caught in the same trap with our caffeine, energy drinks, and chronic stress, which keeps our own nervous systems in sympathetic overdrive. We’re modeling the very patterns we’re trying to help our children overcome.
Breaking Free: A Family Approach to Resetting the Nervous System
The good news is that the nervous system is remarkably adaptable. With the right approach, both you and your children can break free from cortisol addiction and establish healthier neurological patterns. Here’s how:
- Address the Root Cause
Rather than simply masking symptoms, look for approaches that identify and correct the underlying neurological imbalance. Nothing can accomplish that better than neurologically-focused chiropractic care, which is what we do here at Rochester Chiropractic and Wellness. Our INSiGHT Scans can identify areas of tension and interference in the nervous system, which we can use to develop personalized care plans to restore proper function. Each specific adjustment helps release stuck stress, activating the parasympathetic branch and allowing the body to shift out of fight-or-flight and into rest-and-restore mode naturally.
- Create a Home Environment That Supports Parasympathetic Activation
- Establish consistent sleep routines with earlier bedtimes and screen-free wind-down periods
- Reduce sensory overload by creating quiet spaces and scheduled downtime
- Spend time in nature, which naturally promotes parasympathetic activity
- Practice deep breathing exercises
- Limit processed foods and sugars that create blood sugar instability and stress
Your Family’s Path Forward
If you recognize your family in this story, take heart. You’re not alone, and there is a path forward. The first step is understanding that what you’re experiencing has a physiological basis—it’s not a parenting failure or a character flaw in your child.
By addressing the root neurological causes of cortisol addiction and making supportive lifestyle changes, you can help your entire family break free from the stress cycle and discover what true balance feels like.
Imagine what life could be like when:
- Your child can focus when needed and relax when appropriate
- You have natural energy throughout the day without constant stimulants
- Bedtime becomes peaceful rather than a battle
- Your family enjoys time together without the constant undercurrent of stress
This vision isn’t just a fantasy—it’s entirely possible with the right approach. Your family deserves to thrive, not just survive. The journey to neurological balance starts with a single step, and that step is understanding what’s really happening beneath the surface of those challenging behaviors and exhausting days.
Don’t wait to schedule an appointment at RCW for a consultation. If you are not local to us, check out the PX Docs directory to find an office near you.
You have more power to change your family’s health trajectory than you might realize. The time to start is now!





